
Citation: Brown TJ. The Ethical Dimensions of Incivility in Nursing Education. Nurs Health Care Int J 2017, 1(3): 000118.
*Corresponding author: Tamara Jessica Brown, La Salle University, USA, Tel: (732) 773-6163; Email: tjbrown1987@aol.com
Incivility is increasingly being reported within nursing education. This essay identifies and discusses relevant morals, values, and ethical issues presented by incivility as they apply to all valid stakeholders. Ethical theories in the ethical decision-making process are deliberated individually. Within the examination of each ethical theory, ethical principles and values are discussed regarding all stakeholders. The relevance of incivility to the health profession of nursing and how such behavior affects health care services in general is presented. It concludes by determining the desired outcomes, interventions available, and a recommendation for how the ethical issue should be resolved
Keywords: Breastfeeding; Lactation; Suckle; Boosts
It was 8:30 am in the morning just as nursing classes had begun when 41-year old Robert Stewart Flores Jr. entered the University of Arizona’s College of Nursing building with his back-pack strapped to his back. Most students were taking midterms. Flores was a thirdsemester nursing student. He had been divorced, a father of two children, and had been experiencing financial difficulties related to child support payments. He had failed three courses the previous semester. Flores proceeded to the second-floor office of the Assistant Nursing Professor Robin Rogers and shot her multiple times killing the 50-year old. He then ascended to the fourth floor where a class of students were 40 minutes into an exam. He aimed his gun at Cheryl McGaffic who was sitting in the front of the classroom to whom he called out her name and stated, “I’m going to give you a lesson in spirituality,” after which he shot her in the chest two times. Another instructor of the course who was standing at the podium when Flores entered, Barbara Monroe, witnessed this shooting and fell to the ground to curl beneath a desk. Flores moved over Monroe and asked her if she remembered the last thing she said to him to which she replied. “No”. He then asked her, “Are you ready to meet your maker?,” before shooting the 45-year old three times. Rogers, McGaffic, and Monroe were the nursing professors of the courses Flores had failed the previous semester. He had been barred from taking the exam his classmates were finishing and would later turn the gun on himself taking his own life. The troubled student had mailed a detailed plan of his attack prior to the killing [1].
The aforementioned vignette is a true story and tragic example of incivility. Based on the work of several civility scholars, Clark developed the following definition of incivility: “Rude or disruptive behavior which often result in psychological distress for the people involved- and if left unaddressed, may progress into threatening situations” (2009, p. 194).Uncivil behaviors contribute to school avoidance, absenteeism, decrease in grades, students’ inability to concentrate, loss of interest in academic achievement, and increased withdrawal rates [2]. When incivility disrupts the academic environment, it is called academic incivility. Academic incivility can occur anywhere teaching and learning may occur including a school campus, a student lounge, hallways, offices, online classroom. Anywhere a ‘teachable moment’ for a civility discussion may occur, incivility has the potential to happen [3].
Uncivil behavior exists on a continuum with disruptive behaviors on one end and threatening and violent behaviors on the opposing end. Such behaviors may be intentional or unintentional in that individuals may be unaware of the effects of their behavior or speech on others. On the low-risk end of this continuum are distracting, annoying, and irritating behaviors such as eye-rolling, sarcastic comments, bullying and taunting. The high-risk end consists of aggressive and potentially violent behaviors such as racial/ethnic slurs, intimidation, physical violence, and tragedy-as the aforementioned happening at Arizona University.
Incivility may be in the hands of students or faculty. Incivility may occur in a variety of patterns: student to student, faculty to student, student to faculty, or faculty to faculty. Clark (2013) [3] describes that the effects of uncivil encounters result in a “dance of incivility”. The dance is interactive in nature meaning that is a process of giving and taking. All participants in the academic environment are affected and therefore are responsible for the creation of a civil academic environment. She explains the metaphor of incivility as a dance emphasizes the “reciprocity and interrelationship that might exist among faculty, students, and administrators when incivility occurs” [3].
The evidence has shown that incivility is a moderate problem in nursing education in both the academic in hospital environments. It ranges from verbal abuse to physical violence. Both faculty and students often express concern that they do not know how to properly address such behaviors. A survey completed at one university asked participants to report their perceptions of incivility among students and faculty. About 70 percent of its nursing students and about 90 percent of its nursing faculty participated in the study. Both groups reported uncivil behaviors. Faculty most frequently reported the following uncivil behaviors in students: “included making disapproving groans, making sarcastic remarks or gestures, not paying attention in class, dominating class discussions, using cell phones during class, and cheating on examinations” [4]. Nearly 100 percent of faculty in one survey reported tardiness, talking in class and other inattentiveness by students. About 50 percent of the subjects in the survey had reported being yelled at during a class or at a clinical setting. There are reports of even more frightening behavior by students including being pushed, having objects thrown at them, their personal belongings being vandalized, being stalked and receiving death threats [5].
Students most frequently reported the following uncivil faculty behaviors in the aforementioned survey including: “canceling class without warning, being unprepared for class, not allowing open discussion, being disinterested or cold, belittling or taunting students, delivering fast-paced lectures, and not being available outside of class” [4]. Faculty are not the only individuals who are reported by students as behaving in an uncivil manner. Nursing students have also reported disrespectful and devaluing behavior by fellow students and clinical agency staff [5].
The Morality of CivilityIncivility in the academic environment blatantly undermines morality-specifically respect for all persons, including student nurses, nursing faculty, and the campus community. Respect for persons is a central concept of many ethical theories. Some ethical theories actually hold this concept as the essence of morality and foundation of all moral duties. Likewise, civility, the opposite of incivility, requires “an authentic respect for the people involved and that each encounter requires time, presence, engagement, and intention to seek common ground” [3]. Conversely, incivility undermines this principle of respect. It is defined by Emry& Holmes (2005) [6] as “disregard and insolence for others, causing an atmosphere of disrespect, conflict, and stress”.
Much of the literature that describes a safe learning environment does not focus on the elements of a psychologically safe learning environment. In order to change what a person knows, you must allow them to engage in critical reflection. In order for one to engage in critical reflection, a trustful atmosphere must exist where learners are able to make mistakes without apprehension about undergoing negative consequences [7]. To communicate effectively within the learning environment, respect must be present in all parties. Likewise, devoid of respect, learning communities cannot be built, neither can high-functioning health care teams be created. College classrooms can still become engaged in lively debate and spirited discussion without censorship. Civility allows decorum to be added to discourse among students and faculty. The academy must create and sustain a culture of civility so that members of a campus community feel safe to express themselves without discrimination, harassment, threats or intimidation. In the promotion of civility among nursing students and nurse faculty, nursing education play a crucial role in promotion of respect and civility in both the academic and clinical settings [3].
Relevance to Health ProfessionIncivility and its Stakeholders: Incivility in nursing education has numerous stakeholders that must be carefully considered including: faculty, clinical nurse educators, nursing students and their loved ones, the campus community, patients, the nursing profession, healthcare professionals, healthcare organization, society and the public, state boards of nursing, and other public health and nursing organizations. We will explore each of the stakeholder’s unique outlooks by applying ethical theories to how they are affected by incivility in nursing academia. The ethical theories that will be discussed in the context of nursing education incivility will be teleology (consequentialism), utilitarianism, deontology (Kantianism), virtue ethics, care ethics, pragmatism, natural law theory, and egoistic theory. Within such discussions, various values and the ethical principles of beneficence, non-maleficence, fidelity, and justice will be applied as well. A “top-down” ethical analysis of incivility in nursing education will occur throughout the discussion. This approach looks at a credible moral theory and examines a case from the perspective of that moral theory [8] (Table 1).
ConsequentialismHealthcare organizations, nursing organizations, patients, and the public nursing professionals serve find concern with incivility when the incivility experienced by or from nursing students or as the nurses they become begin to affect patient outcomes. The Joint Commission issued a sentinel event alert on this subject in July 2008 with a go-live date of January 2009. It noted that health care settings are high stakes and pressure packed that test the limits of workplace civility. Therefore, it recognized that discourteous and disruptive behavior of heath care professionals can threaten patient safety, the provision of quality care, and employee satisfaction. In an effort to address these behaviors, both covert and overt in nature, TJC disseminated a new leadership standard (LD.03.01.01). TJC makes it clear that “uncivil, disruptive, and intimidating behavior in health care can lead to medical errors, poor patient care and satisfaction, preventable adverse patient outcomes, and increased costs of care. Incivility also causes qualified clinicians, administrators, and managers to seek new positions in more professional environments” [3].
The State Boards of Nursing are also beginning to injunction schools of nursing for the incivility of students, faculty, and practice partners. One school of nursing could have been closed if it did not produce a set of ‘expectations, interventions, strategies, and written policies to improve its culture of academic civility’. They were also expected to generate evidence of a respectful, trustworthy, constructive, and productive academic atmosphere as well as enhanced student-faculty relationships and interaction and communication that safeguarded student success [3]. As authority organizations over the nursing profession and academia, nursing professional organizations and state agencies are responsible for ensuring the safety of patients, the wellness of nursing professionals, and nursing students.
State and local educational agencies are required to report to state and federal agencies their compliance with applicable laws and regulations regarding anti-bullying policies. The basic aspects of such policies that must be upheld on school campuses must include a purpose statement; statement of scope; specification of prohibited conduct; enumeration of specific characteristics; development and implementation of policies and their components (such as definition of bullying; the procedure for reporting; investigating, and responding to bullying; written records of incidents; sanction;, and referrals); review of local policies at a set time period, communication planning, training and preventive education, transparency and monitoring, and a statement of rights to other legal resources. The policy and procedure regarding incivility (i.e. bullying) exhibits an important aspect of procedural justice. Schools of nursing and their universities must create a procedure for students, their families, faculty, and other staff to report incidents of incivility in a way that is anonymous, if needed, and which will protect the reporter from retaliation. Also this aspect of the policy would also have to designate the school personnel responsible for receiving reports and who will respond in a timely and responsive manner (http://www.stopbullying.gov/laws/keycomponents/index.html).
Pragmatism: A Contrast to ConsequentialismConsequentialist moral theories evaluate the morality of actions in terms of advancement to a goal. The goal of regulatory agencies such as TJC and BON is a culture of academic civility. The faculty unknowingly practicing uncivil behavior may rationalize that her methods are done in an effort to ensure students understand the magnitude of their practice or to prepare them for the ‘bullying’that will occur in the workplace. They may speak based upon ethical theories such as deontology, virtue ethics, and natural law. They may have a pragmatic theoretical outlook which “maintains that rightness of actions is determined by what works or is most useful”. They may have practiced in such a way for years and their students have gone on to success in the nursing profession. Nevertheless, the consequentialist sees the intent of such a faculty member as irrelevant to whether an action is right or wrong. Outcomes are the sole concern of the consequentialist. The consequentialist ethical theory applies to patients, the public, the nursing profession, healthcare professionals and organizations, society, and regulatory agencies.
UtilitarianismClassic utilitarianism is based on the net benefit of an act. Rule consequentialism allows for the decision maker to develop rules that will have the greatest net benefit. Civil environments are the foundation for [the net benefit of] safe patient care and optimal outcomes. Likewise regulatory nursing agencies and healthcare organizations are obligated to the public to ensure that the care provided by nursing professionals and healthcare professionals is safest and of the highest quality. In doing this, they are able to uphold the ethical principles of beneficence, non-maleficence, justice, fidelity to protect public health.This responsibility is allotted to these authorities due to deontological ethics theory.
Healthcare organizations also are valid stakeholders in this issue. Pearson and Prath (2009)[9] found that 95% if American workers report experiencing incivility from their coworkers. As a result, workers report they become actively disengaged and less productive. Some participants even went on to report they intentionally undermine their organizations and their coworkers. The impact of one uncivil employee can be costly when one includes the cost associated with supervising the employee, management of the situation, consultation with attorneys, and interviewing those who witnessed the episode including doctors, nurses, patients, and others. In one case, a hospital lost more than $25,000 as a result of an uncivil episode. Simon (2006) [10] estimates that an individual episode of incivility may range in cost from $30,000 to $100,000, when employee benefits, retention and recruitment expenses are included. Hospitals already are challenged to retain nurses. Failed recruitment and retention are what drain health care organizations financially. Negative outcomes associated with incivility include absenteeism, poor quality of care provided and subsequent negative patient outcomes, which then causes nurses to not only leave their jobs but the profession as a whole [11]. The Workplace Bullying Institute (2010) [12] projects the annual cost of United States organizations to be an approximated $300 billion.
The greatest stakeholders of incivility are patients that exist in the public and the communities nursing professionals serve.A common theme that is threaded throughout the American Nurses Association (2001) [13] and the International Council of Nurses (2006) [14] codes of ethical nursing practice is the importance that “the patient is the central focus of a nurse’s work and that they are to protect the moral environment in which patients receive care” [15]. The two key principles that exist as the underpinning of ethical practice in nursing and healthcare are those of beneficence and non-maleficence. Nurses have an obligation to do good and to avoid doing harm. Fry (2008) explains that nursing professionals acting on these principles mean helping others gain what is beneficial to them and practicing behavior that will prevent or decrease the risk of harming patients physically or psychologically. Nurses who behave uncivilly often bring such behavior to the bedside so that patients may not feel respected. Patients are also affected by the unsafe care provided to them when rather their nurses or nursing students taking care of them are the recipient or perpetrator. Incivility increases the stress and frustration of nurses. Rosenstein and O’Daniel (2006) surveyed 244 subjects at one hospital and compared their responses to national research database of 4,000 nurses physicians, and administrators who responded to the question, “Are you aware of specific adverse events that did occur as a result of disruptive behavior?” Nationally, 14 percent of those who responded answered “yes” compared to the 19 percent of the hospital sample and 46 percent at a comparison hospital. The subjects related uncivil behavior to the occurrence of adverse events (67 percent), medical errors (67 percent), compromises in patient safety (58 percent), impaired quality of care (68 percent), and patient mortality (28 percent).
Teleology and DeontologyFrom a deontological perspective patients expect nurses to perform their care safely and equally. Nurses and nursing students have a duty to provide the best care possible to their patients. Likewise, nursing faculty have a duty to provide the best education to nursing students, the parents who invest in such education, and the public who will become the recipients of their care. A nurse may not be able to perform consistently and practice justice or distributive justice. For example, a nurse may experience an uncivil behavior one shift, which adversely effects the quality of her work. In contrast, if the same nurse was exposed to civil behavior another shift, the quality of her work would have the opposite effect. Patient outcomes are affected by how nursing professional behave with other healthcare professionals, themselves, and nursing students. Nurses are likewise a valid and important stakeholder as the care they provide may be affected by acts of incivility. If an error is made, they may lose their license to practice and subsequently their livelihood.
The teleogical perspective of utilitarianism theory is based on the idea that moral rightness of an action is determined by the balance of good and bad consequences of that action. Nurses must be able to practice in a fastpaced highly stressful working environment without incivility. When nurses encounter incivility like bullying in the workplace, they report an increase in distraction and disruption of concentration. This issue also affects human factor areas of collaboration, communication, and teamwork. Incivility only adds to the pressure as nurses work to fulfill their duty of fidelity to protect public health [16].
Nursing students do not only encounter incivility from nursing faculty but also nursing professionals they encounter in their clinical experiences.
Nurses make up the largest number of the health care population, and therefore have the position to lead change within the healthcare system. The Institute of Medicine Report (2010) [17] has called on nursing to increase their leadership capacity and participate in implementing transformational change in health care. They must do so to redefine the future, bring together people, and inspire action to create a convincing vision and see that meaningful results occur. Their report had four key messages:
1. Nursing should practice to the full extent of their education and training
2. Nurses should achieve higher levels of education and training through an improved education system that promotes seamless academic progression.
3. Nurses should be full partners, with physician and other health professionals, in redesigning health care in the United States
4. Effective workforce planning and policymaking require better data collection and information infrastructure.
To reinforce these key messages, the IOM report presented eight recommendations. Three of these recommendations are relevant to the issue of incivility:
Recommendation 2: Expand opportunities for nurses to lead and diffuse collaborative improvement efforts
Recommendation 7: Prepare and enable nurses to lead change to advance health
Recommendation 8: Build an infrastructure to collect and analyze health care workforce data (p. 59-62).
These recommendations provide the rationale for adopting a culture of civility among all healthcare professionals. There is a need for collaboration, teamwork, and collegiality among healthcare professionals. In order for these goals to be met, civil and respectful relationships must be established. Healthcare professionals are stakeholders because they must work with future and current nurses in creating a healthcare system that “makes quality care accessible to the diverse populations of the United States, intentionally promotes wellness and disease prevention, reliably improves health outcomes, and provides compassionate care across the lifespan” [17].
The Institute of Medicine’s (2010) [17] report likewise highlightedthe greater professional responsibility of nursing education to adequately prepare the next generation of nurse leaders. Incivility by faculty contributes to the attrition of nursing students. Likewise incivility by students contributes to the attrition of nursing faculty. The attrition is due to victims not being able to face entering the uncivil situation and not having the resources to combat the incivility.
Nursing student and faculty attrition is a special concern due to the shortage of registered nurses and nursing faculty in the United States. According to the Bureau of Labor Statistics’ Employment Projections 2012-2022 (2013) [18], there is a projected need of 525,000 replacement of nurses in the workforce. This brings the total number of registered nurse job openings for nurses to more than 1 million by the year 2022 due to job growth and replacements. The American Association of Colleges of Nursing [19] explains that United States schools of nursing turned away over 70,000 qualified applicants from baccalaureate and graduate nursing programs due to there being an insufficient number of faculty available among other reasons such as limited clinical sites, classroom space, preceptors, and budget constraints. However, greater than 60 percent of the nursing schools specified that the shortage of faculty was the reason qualified applicants were not accepted into entry-level baccalaureate nursing programs. These shortages are predicted to only grow larger in the next decade [20].
In the March-April 2005 issue of Nurse Economic$ Buerhaus, et al. [21] found that 75 percent of registered nurses believed that the impending nursing shortage will be a major problem for “the quality of work life, the quality of patient care, and the amount of time nurses spend with their patients. ” When asked how the shortage will affect the future of the nursing profession, most respondents saw it as a catalyst for increasing stress on nurses, lowered patient care quality, and a cause for nurses to leave the profession.
Not only does incivility cause the potential for harm to be done to patients but also healthcare professionals themselves. Incivility or bullying have long lasting effects such as physiological symptoms, anxiety, nightmares, decreased self-esteem, and the use or abuse of alcohol or drugs to cope. Nursing professionals,whether clinical nurses or faculty, suffer from incivility from each other. Faculty also suffer incivility from students. However, student nurses not only are the victims of incivility from faculty but also from working nurses. During clinical rotations, Randle (2003) [22] found 90 percent of nursing students reported experiencing negative interactions with nursing staff. Such behavior included negative criticism, bitterness, public degradation, and passive bullying. Preceptor conflict during these interactions left nursing students feeling vulnerable, ignored, powerlessness, stressed, and suffering from a negatively altered selfimage. In an effort to be accepted, students tolerate such behavior [23]. Such socialization to the profession is unacceptable when one considers the negative emotional effects of such behavior. The ethical principles of beneficence and non-maleficence of all parties involved are clearly violated in light of this issue.
Virtue EthicsVirtue ethics is a broad term for a theory that focuses on the roles of character and virtue. This is in contrast to doing one’s duty or acting in way that brings about good consequences. According to this theory, a virtuous person does what is good or upright in many situations throughout their lifetime due to the nature of one’s character -rather than to maximize utility or to perform a duty. The aim of this theory is to identify universal principles that can be practical for any moral situation [24].
A focal virtue is compassion. Compassion combines “an attitude of active regard for another’s welfare with an imaginative awareness and emotional response of deep sympathy, tenderness, and discomfort at the other person’s misfortune or suffering” [25]. This virtue is the ability of one to imagine one’s self in another’s situation. Oftentimes a patient’s need for compassionate care outweighs the technical part of care needed. Moral subjectivism and ethical egoism are important in having compassion for both the role of nursing student and nursing faculty member. Both roles have inherent stress associated with them and if both parties make an effort to understand these, they may act in a more compassionate and civil manner.
Care EthicsCare ethics is a theory which falls within the domain of virtue ethics. Care ethics is a moral theory which “implies there is a moral significance in the fundamental elements of relationships and dependencies in life”. It normatively has a purpose of maintaining relations “by contextualizing and promoting the well-being of care-givers and carereceivers in a network of social relations”. It is often considered a virtue or practice that looks to meet the needs of one’s self and others- particularly those who are dependent and vulnerable [26].
In the clinical nursing education environment, students have the opportunity to work in a variety of clinical settings alongside professional nurses. Such clinical environments often are unstructured, unpredictable, and overwhelming which often generate feelings of vulnerability among students. Cahill asserts that the relationship between nursing staff and the nursing students is the single most important factor that creates a positive learning environment in this particular setting. Nevertheless, poor treatment of nursing students is common in the workplace. This is due to a shortage of nursing staff, increased workload, lack of teaching competency, and staff feeling threatened by nursing students. Students often report hostility, disrespect, or being completely ignored by nursing staff. As a result, they are unable to engage in necessary communication which would further their learning activities and goals.
Nursing students most commonly develop their personal professional behaviors in the context of patient care through role modelling. When nursing students observe their professors and nursing professionals interact with themselves, their patients, and each other, they use what they observe and determine how they will create their own understanding of the patient’s world and the role they will play in it. The nurse who adopts teaching responsibilities facilitates this process for the nursing student by facilitating the development of their professional behaviors and identity. Therefore, the outcomes of role modeling may be negative and positive. Positive behaviors are those that facilitate desirable professional development of the learner. Negative behaviors are those that are unprofessional, unethical, and inappropriate. Role modeling is greatly reliant on imitation and observation. Therefore the student may easily adopt either of these behaviors. Students are vulnerable in this way to the behaviors they observe in the academic and clinical settings of nursing education [27].
As role models, incivility of nursing faculty actually plays a contributing factor to student incivility. Kolanko, et al. (2006) [28] explain that the consequences of faculty incivility includes damage to the mentoring role that faculty have a duty to provide, problematic learning environments, increased likelihood of violence, and greater stress in student relationships with families and friends.
Egoistic TheoryNursing is known in the literature as the profession that ‘eats its young’. How can the caring profession be so insensible? When incivility flourishes, this only reinforces the trend of older, experienced nursing professionals being hostile towards its novices. This disruptive behavior tarnishes the image of academic nursing education and the nursing profession. It also has the potential to leave only the perpetrators of such behavior as the only individuals working in the profession. Egoistic theories posit that what is right is what maximizes an individual’s self-interests. Nevertheless, as health care professionals, a fiduciary relationship is had with patients. Patients can trust that healthcare professionals always place that patient’s interest ahead of their own. Therefore it is an imperative task for all parties involved to ensure that incivility is limited if not altogether eliminated.
Natural Law TheoryNatural law theory posits that the rightness of an action proves self-evident in the laws of nature which is orchestrated by the supreme law-giver, God. The morality of an action not determined by customs or one’s preferences. Rather, it is commanded by the law of reason which can be seen in nature and human intellect. Any view that is contrary to the views of the laws of nature is immoral. Therefore, it stands to reason that humans would provide a natural response to Incivilbehavior that would dictate such behavior good or bad. Students and faculty report emotional responses to incivil behavior, including feeling “traumatized, helpless, powerless,diminished self-worth, self-doubt, and anger” [29].
Within natural law theory, the Golden Rule or the ethic of reciprocity states that one should treat others as they would like to be treated. Its corollary is the Silver rule which focuses on restraint and states that one should not treat another as you would not like to be treated [30]. There is no doubt that neither students nor faculty would like to be treated in such a debased way. Any action that degrades a human being is considered unjust from this ethical outlook. Therefore, incivility in nursing education clearly violates natural law theory’s view of morality.
ConclusionThe public is concerned about the best outcomes for themselves and their loved ones. Healthcare professionals including nurses wish to work in health and fulfilling work environments void of conflict and disruptive behavior. Likewise, nursing students and clinical faculty who enter the clinical and academic setting wish to work collaboratively with health care professionals and benefit from positive role models and mentoring relationships. As they prepare the next generation of nurses, nursing faculty wish to work in a collective effort to elevate the edification of students and themselves. Regulatory and professional organizations of nursing have a vested interest in ensuring the academic and clinical realm of nursing is free of any influence that could adversely affect patients or the quality of care provided by nurses. The consequences of these desired outcomes make the case for a superior and urgent goal.
Incivility is unacceptable wherever it occurs and to whatever degree it occurs, rather it is a rolling of the eyes or blatant violence. It has no place in nursing. This negative behavior must be acknowledged in nursing. It must not be ignored. It has significant consequences for the socialization of the student nurse and new graduate nurse to the professional nursing role. Incivility must be taught in nursing curriculum and professional workshops so students, nurses, and faculty know how to address such behavior and not face it unprepared. Therefore, procedural justice will occur in such situations. Students must be empowered to stand up to such abuse. Campus universities, schools of nursing, healthcare organizations, and regulatory agencies must support an environment that has zero tolerance for such disruptive behavior. Research has found an association between such policies and the prevention of incivility. As a result, we retain nurses and nurse faculty during the dawning nurse and nurse faculty shortage [31] Ultimately, patient safety is upheld and the psychological well-being of healthcare professionals [32], students, and faculty are safeguarded. Nurses, rather students, faculty, or clinicians, must be empowered with skills to combat such behavior and trust their employers and schools will step in to protect incivility from ever occurring. None of the stakeholders involved deserve to be a victim of incivility.
As this discussion concludes, the most important value nursing and nursing education must uphold is that of integrity, or maintaining the wholeness of character of nurses individually and the profession as a whole. According to the American Nurses Association’s Code of Ethics for Nurses with Interpretive Statements (2001) [12], integrity is maintained by actions occurring which are consistent with personal values and those of the nursing profession. Due to constraints and the self-serving nature of individuals, groups, and organizations, the integrity of nurses are threatened and may present itself as a serious pitfall. Nursing students and faculty may be subject to uncivil conduct , emotional or verbal abuse, and may lash back with similar behavior. Nevertheless nursing students and faculty must “guide moral reasoning and actions, even when other people challenge the nurse’s beliefs” [15]. A nurse faculty member stated: “If nursing is a caring profession, what does uncivil behavior among students and faculty say about us? What does it say about future generations of nurses? We must do better.” [33]. Similarly a student voiced his concern in the form of a question: “How can the nursing profession preach the importance of caring when nurses ignore or sacrifice ethics, justice, and personal integrity for their own gain?” [29].
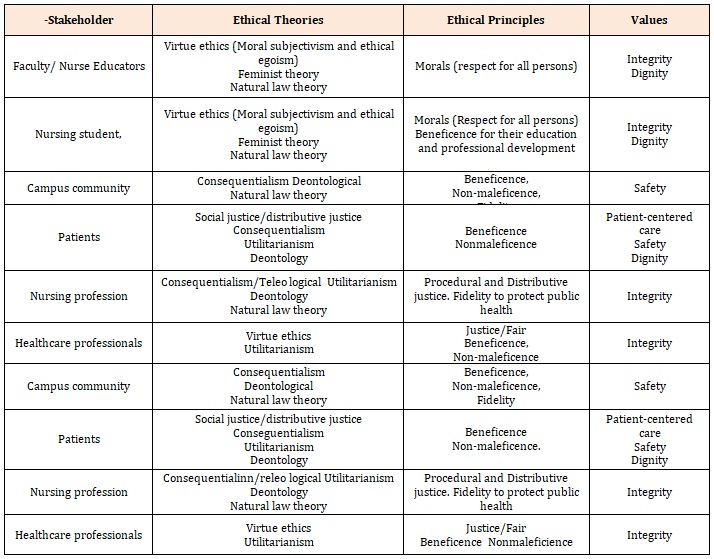
Table 1: Stakeholders, Ethical Theories, Ethical Principles, and Values Concerning Incivility in Nursing Education.
Chat with us on WhatsApp



